
Good news can be hard to believe
Healthcare stories from this week.

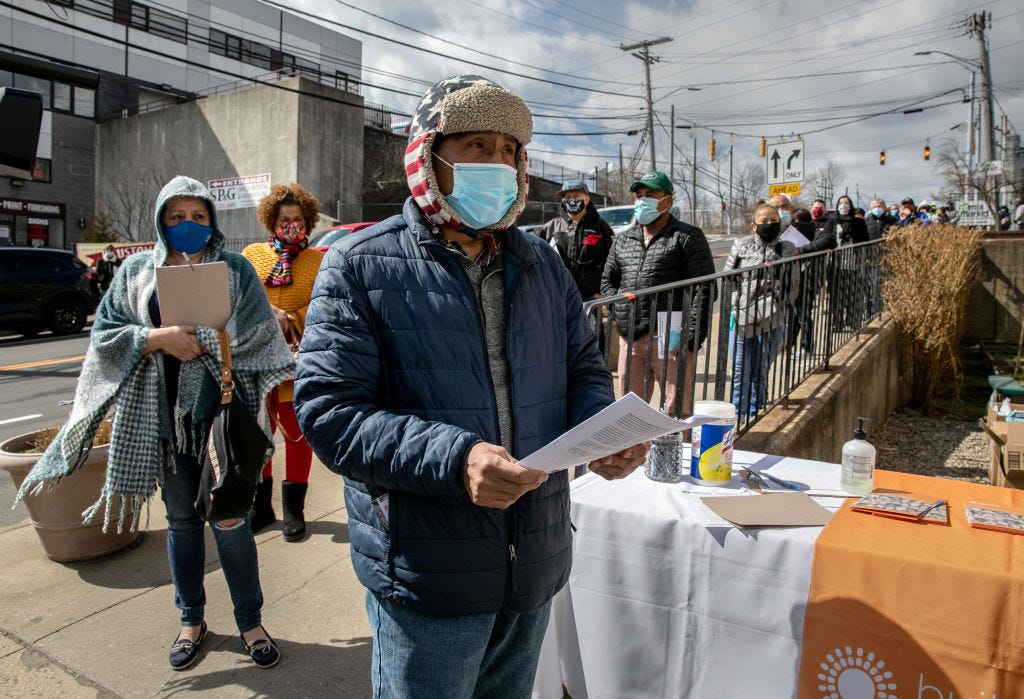
The Fresno Bee had an excellent article this week about the proposed expansion of Medi-Cal, the difficult-to-Google Medicaid program in California, to all undocumented immigrants. This would be a major new source of coverage for over 700,000 undocumented people who currently qualify for neither Medi-Cal nor marketplace coverage. (Newsom already expanded Medi-Cal to undocumented immigrants over the age of 50, who will become eligible in May, and people under 26 are already eligible.) Two thirds of undocumented immigrants in California under 65 are uninsured. Aside from some very limited local programs around the country that mostly focus on children, it’s much harder for the undocumented to get health insurance at all, let alone to afford it.
An important fact that I learned a few years ago and never forgot, unlike most things I learn: Immigrants in the United States pay more in private insurance premiums than they receive in health spending, effectively subsidizing healthcare for native-born Americans, according to a 2018 study in Health Affairs. (The same is true for Medicare, according to another 2018 study.) The researchers found undocumented immigrants generated a bigger per-person subsidy than legal immigrants or native-born Americans; insurers spent $4233 per native-born American, versus just $1781 per undocumented immigrant. The authors suggested that this gap might be due to immigrants’ “relative youth and good health, as well as the reluctance of many to seek care.”
Which brings us back to the California proposal. If it goes into effect, it would be a truly massive change for undocumented people. But it must come with a similarly huge effort to educate immigrants of their new rights, to overcome years of damage done by policies with the exact opposite intent.
Sergio Tulio Arévalo Soliz, an undocumented farmworker interviewed for the Fresno Bee story, “waited to seek medical care for his heart condition until he could no longer handle the pain.” That condition led to emergency heart surgery, which put him out of work for months—one of the reasons workers like him avoid going to seek care in the first place. These are unavoidable choices that low-income people in America, citizens and non-citizens alike, have to make; they can’t afford to be out sick, so they work until they can’t. But it’s even worse for undocumented people who, on top of the financial pressure, are often terrified of being deported if they seek medical care. In a New York Times piece from March 2020, immigrants in another California farming community expressed fear that going to the hospital for Covid-19 might lead to deportation, or hurt their chances of permanent residency.
(A quick aside, just to be clear about terms, because I encounter a lot of confusion about this: You can be lawfully present in the US without being a permanent resident, like if you’re on a work visa. Someone who is approved for permanent residency—sponsored by work or an American citizen immediate family member, not through just being here for a certain number of years—gets a “green card.” A permanent resident is not a citizen, but will be eligible to apply for citizenship after a certain number of years.)
There’s no better recent example of this dynamic than the Trump administration’s heinous ‘public charge’ rule, which expanded the categories of public benefits that could disqualify immigrants from obtaining permanent residency to include Medicaid, as well as SNAP (food stamps) and public housing. News of that rule frightened people—even those already with a green card—away from applying for benefits they were legally entitled to, long before the rule was implemented. As soon as it was proposed, stories began to emerge about frightened immigrant mothers dropping WIC benefits that helped them feed their children. That rule was an expansion of a long-standing feature of the immigration process that discourages immigrants from using public programs. When I married my American husband and applied for a green card, he had to sign a form saying he’d pay back the government if I used Medicaid or other public programs—even if we got divorced. (Thanks, sweetie!)
Of course, this rule was never really intended to do anything but terrify immigrants and discourage them from seeking any help at all. Very few people applying for permanent residency would have ever been eligible to get on Medicaid, for example. You can’t qualify for Medicaid with a green card until you’ve had one for five years (except if you’re a pregnant woman or child in a slight majority of states, plus some other exceptions). But it was very efficient at creating that chilling effect.
In California, undocumented children have been eligible for Medicaid since 2016, but their enrollment has been trending downwards since Trump took office, even as overall Medicaid enrollment increased during the pandemic. It’s now down to 118,000, from a high of 134,000 in 2017. Even months after the Biden administration rescinded the public charge rule, the hesitancy lingers: A Brookings post from last week cites recent polling showing that almost half of immigrants didn’t apply for benefits they needed during the pandemic because they feared the consequences for their immigration status. As the post argues, there is a lot more the administration could be doing to get the word out. (Given Biden’s record thus far on immigration, don’t hold your breath.)
American immigration bureaucracy and policing is thoroughly cruel and arbitrary: It locks up citizens, deports millions for minor infractions, imposes completely insane standards on immigration applications (which you can only submit on paper, and might end up in a man-made limestone cave under Kansas). I wouldn’t blame an undocumented person in California for being afraid to use a new benefit; after all, it’s a complete reversal of the usual direction of American government policy towards undocumented immigrants and benefits. Undocumented people can’t even buy insurance without subsidies on the ACA marketplaces, under a law passed only 12 years ago, by an administration Joe Biden was part of. The idea of preventing immigrants from accessing our shitty welfare programs doesn’t just go back to Trump, or Obama, or Clinton’s welfare rules; it goes back centuries.
If Newsom’s proposal goes into effect, it will be a truly huge expansion of health insurance, and major milestone in the fight for more humane treatment of immigrants in this country. But it’ll be no wonder if a population that isn’t used to good news from the government takes a while to believe it’s true.

Some more healthcare stories from this week:
This week, there was a great guide to the history and future of Medicare Advantage at The American Prospect. Medicare Advantage is a really remarkable scam on both the government and patients; like all good scams, it’s complicated and hard to follow, but this article will help you see through the flim-flam.
Lauren Kaori Gurley, one of the best reporters covering Amazon, had a story about the company’s ‘wellness huddles,’ an “infantilizing” new scheme in the company’s ever-growing arsenal of thinly veiled PR moves. Workers are required to watch a video telling them to take care of themselves, eat vegetables, blah blah—anything except forming a union with your colleagues to fight for better working conditions, of course. “It’s for them to cover their asses [in case someone gets hurt],” one worker told Gurley. Death to workplace wellness wank!
A real humdinger in the genre of news outlets reporting on depressing stories of societal degradation as if they’re heartwarming—the worst ones always involve children doing adults’ jobs for free, somehow—courtesy of CBS:
A really good Bill of the Month from NPR and Kaiser Health News, involving a classic American hospital scam: The ‘facility fee.’ A family was charged $858.92 for visiting an emergency room, where almost no medical care was received and the doctor never even showed up. Not only is the fee itself outrageous, but the visit was coded as a Level 3 emergency visit, meaning “moderate severity.” For a small burn on a child’s hand that healed quickly, and was not treated at all. Worse still: The family started receiving collections notices while he was still disputing it.
I could have written a whole ‘nother thing about a couple stories relating to the healthcare staffing crisis this week: In Wisconsin, a legal order temporarily blocked seven employees of one hospital system from taking jobs at another, with the first hospital saying it was only seeking to “protect the community.” Across the border in Minnesota, a 70 year old diabetic nurse was asked to come back to her nursing home, almost a year after she retired, because it couldn’t staff its Covid-19 unit. Not only that, she actually did it, too. I hope someone brings her a damn hotdish. But taking the dystopian gold medal, we go back to California, where a newly filed ballot measure that could bring the gig economy to nursing. That’s right: It would be “Uber for nursing.” I am begging California to stop doing these ballot measures.
I group these stories together because they’re all about the staffing crisis, but they demonstrate another thing to me, too: The increasing desperation to solve the problem without giving workers anything. How can we fix this without improving things? We’ll sue them if they try to leave; we’ll call in the diabetic retirees; we’ll switch to contractors.
The exodus of healthcare workers is of course partly due to the horrors of so many patients dying, but it’s also because their employers won’t address pay and working conditions, even as they are in crisis. Why would hospitals rather pay a travel nurse as much as a cardiologist than invest less in nurses who will stay there for years? How could we end up with hospitals hiring their own nurses back as travel nurses at higher rates? There’s no rational business sense at work here; it certainly doesn’t seem profitable to me to grind your experienced nurses out of the business and replace them with more expensive ones who don’t know where the bandages are kept.
I suspect it’s a different impulse, the same one that prevents all those chain restaurant owners from improving working conditions even as it becomes impossible to find any staff at all. It’s a war of owners against workers, and they want to win, whatever the cost—perhaps because they believe maintaining that dominance is the only way to ever-escalating profit and executive salaries in the long run. They want to show that they don’t have to address pay or conditions, because they’re willing to do a dumber, deadlier, more expensive thing instead. If they concede a little, that would show healthcare workers they had power—power they could use again, when the pandemic subsides and they’re wondering why a hospital CEO needs to make 300 times what a nurse makes. I can’t explain it any other way, not even through the profit drive. Maybe, like elephants, hospital leaders are just jerks.
And finally, the best healthcare tweet I’ve ever seen:
See you next week.